If you have chronic dry eye and artificial tears are not cutting it, there is a good chance your meibomian glands — not your tear volume — are the real problem. For patients in this category, two in-office therapies dominate the conversation: Intense Pulsed Light (IPL) and LipiFlow. Both target the oil glands along your eyelids. Both are FDA-cleared. But they work through different mechanisms, treat slightly different patient profiles, and carry different price tags.
At EyeCare Center of Orange County, we evaluate every dry eye patient against the TFOS DEWS II framework — the international gold standard for classifying dry eye — before recommending a treatment. Here is how IPL and LipiFlow compare, how we decide which one (or which combination) is right for a given patient, and what you can expect from a specialist evaluation.
Before we get into the mechanics, one important reality check: neither of these therapies is a replacement for a proper diagnosis. A patient with severe aqueous-deficient dry eye driven by Sjögren's syndrome is not going to benefit from IPL the way a patient with rosacea-driven MGD will. Matching the treatment to the root cause is the single most important step — and it is the step that is most commonly skipped in a standard eye exam.
What Is MGD, and Why Does It Matter?
Meibomian gland dysfunction (MGD) is the leading cause of dry eye disease worldwide. Your eyelids contain roughly 25–40 vertical glands per lid that produce meibum — the oily layer that seals the watery tear film and prevents evaporation. When these glands become plugged, inflamed, or atrophied, your tears evaporate faster than they can be replaced. The result is burning, fluctuating vision, redness, and a gritty sensation that artificial tears can only temporarily mask.
This category of dry eye is called evaporative dry eye, and it accounts for the majority of chronic dry eye cases. Eye drops add water to the surface. They do nothing to restore the failing oil layer. That is why so many patients report that drops stopped working — or never really worked in the first place.
How We Confirm MGD
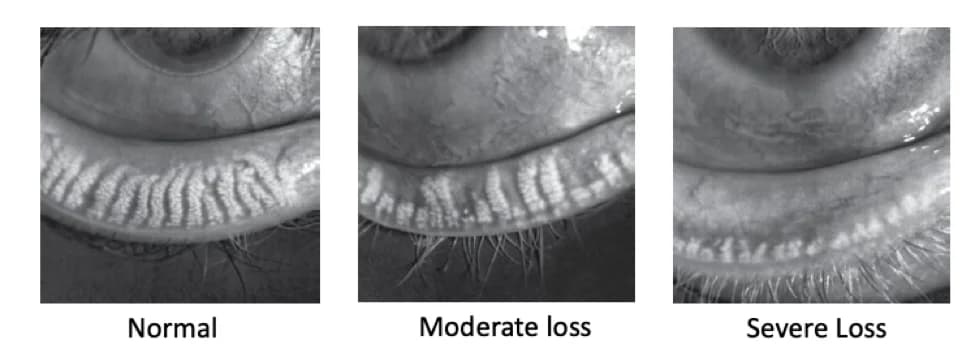
A specialist evaluation should include meibography — a specialized imaging test that visualizes the structure of your meibomian glands. Healthy glands appear as long, straight, parallel tubes. In MGD, they shorten, twist, drop out, or disappear entirely. Without meibography, MGD is easy to miss on a standard eye exam. We also measure tear break-up time, tear osmolarity, and perform a graded lid margin exam so that the severity of gland compromise can be staged against the TFOS DEWS II severity scale. Staging matters because it directly drives the treatment intensity we recommend and the realistic expectations we set for how much improvement is possible.
How IPL Works
Intense Pulsed Light (IPL) therapy was originally developed in dermatology for treating rosacea and sun damage. Ophthalmic research then showed that the same broad-spectrum light pulses, when applied to the periocular skin, dramatically improved dry eye symptoms in patients with MGD. The FDA has cleared specific IPL systems for dry eye treatment.
The Mechanism
- Closes abnormal telangiectatic vessels around the eyelids. These dilated blood vessels leak inflammatory mediators into the glands. Shutting them down reduces the chronic inflammation that drives gland dysfunction.
- Heats the meibum so it liquefies and becomes easier to express. Meibum normally has the consistency of light oil; in MGD, it thickens to a toothpaste-like or waxy state.
- Reduces Demodex mite populations along the lash line. Demodex infestation is an often-overlooked contributor to chronic blepharitis and MGD.
- Stimulates cellular repair in the gland tissue over the course of the treatment series.
What the Session Looks Like
A protective shield is placed over each eye. A cool gel is applied to the skin from cheek to temple. The device delivers a series of light pulses — most patients describe it as a warm rubber-band snap. Immediately after the pulses, the provider expresses the meibomian glands to release the newly liquefied oil. The full appointment takes about 20–30 minutes.
IPL is typically performed as a series of four treatments, spaced two to four weeks apart, followed by maintenance sessions one to two times per year. Results build cumulatively across the series.
Who IPL Is Not For
IPL is not appropriate for every skin type. Patients with Fitzpatrick skin types V or VI (darker skin tones) carry an increased risk of post-inflammatory hyperpigmentation and are not ideal candidates. IPL is also avoided in patients with active eyelid skin cancer, recent isotretinoin (Accutane) use, a history of severe keloid scarring, or during pregnancy. We screen for all of this during the evaluation before scheduling any sessions.
How LipiFlow Works
LipiFlow Thermal Pulsation (Johnson & Johnson Vision) was the first FDA-cleared in-office device specifically designed to treat MGD. Rather than using light, LipiFlow uses controlled heat combined with pulsating pressure applied directly to the inner eyelid surface.
The Mechanism
- Heats the inner eyelid to a precise temperature (around 42.5°C / 108.5°F) that liquefies hardened meibum inside the glands.
- Applies gentle pulsatile pressure to the outer eyelid surface, milking the softened oil out of the gland openings.
- Protects the cornea — the device sits under the lid, against the conjunctiva, so the heat is applied from the inside where the glands actually live (not through the skin).
What the Session Looks Like
After numbing drops, a single-use activator is placed under each eyelid. The device runs automatically for 12 minutes per eye, delivering synchronized heat and pressure. Most patients find it surprisingly comfortable. Typically, LipiFlow is performed as one treatment, with effects lasting 9–12 months before a repeat procedure is considered.
Who LipiFlow Works Best For
LipiFlow tends to shine in patients who have heavy, waxy gland obstruction on meibography but minimal telangiectasia and no active rosacea. It is also a strong option for patients with darker skin tones who are not good IPL candidates. Because the treatment is a single appointment, it appeals to patients who cannot commit to the multi-session IPL schedule — though that convenience comes with a correspondingly higher per-session cost.
Head-to-Head Comparison
| Feature | IPL | LipiFlow |
| Mechanism | Light pulses to periocular skin | Heat + pressure directly on inner eyelid |
| Treats inflammation | Yes — closes abnormal vessels | No — purely mechanical |
| Treats gland obstruction | Yes — via heat + expression | Yes — heat + pulsation |
| Best for ocular rosacea | Yes — gold standard | Less ideal |
| Best for Demodex / blepharitis | Yes | No direct effect |
| Number of sessions | 4 initial + annual maintenance | 1 session, repeat in 9–12 months |
| Time per session | 20–30 minutes | ~25 minutes (both eyes) |
| Skin type restrictions | Yes — not for Fitzpatrick V–VI | None |
| Downtime | None — minor redness possible | None |
Which One Is Right for You?
There is no universal winner. The right treatment depends on your phenotype of dry eye, your skin type, your budget, and whether inflammation or mechanical obstruction is the dominant problem.
IPL Is Usually Preferred When:
- You have ocular or facial rosacea, flushing, or visible telangiectasia on the eyelids
- You have chronic blepharitis or a confirmed Demodex component
- You have moderate gland dropout on meibography but the remaining glands are still functional
- You want a treatment that addresses the inflammatory driver, not just the mechanical blockage
LipiFlow Is Usually Preferred When:
- Your glands are heavily plugged but skin inflammation is not a major factor
- You have a darker skin tone (Fitzpatrick V–VI), where IPL is not recommended due to pigmentation risk
- You prefer a one-and-done appointment over a multi-session series
- You cannot take time for four separate treatments over two to three months
When We Combine Both
For patients with advanced MGD, significant rosacea, and severely capped glands, the most durable results often come from IPL first (to quiet the inflammation) followed by LipiFlow (to mechanically express the glands). This sequential approach is increasingly recognized as the standard of care for moderate-to-severe evaporative dry eye.
What Neither Treatment Can Do
It is important to be honest about limits. Neither IPL nor LipiFlow can regrow glands that have already dropped out. If meibography shows that large portions of the gland tissue have atrophied, our goal shifts to preserving the remaining glands and keeping the ocular surface comfortable. For that category of patient, we often add scleral lenses to the plan because they hold a reservoir of sterile fluid against the cornea all day and buy the surface time to stabilize.
Cost in Orange County
Both IPL and LipiFlow are considered elective therapies and are generally not covered by medical insurance or vision plans. Pricing in the Orange County market varies by clinic and protocol, but the ranges below are typical as of 2026:
- IPL: Priced per session, with a full initial series of four sessions and periodic maintenance recommended
- LipiFlow: A single-session treatment covering both eyes, repeated every 9–12 months as needed
We walk every patient through exact pricing, financing options (including CareCredit), and what a realistic one-year and three-year treatment plan looks like before committing to anything. No one should start a multi-thousand-dollar dry eye protocol without knowing exactly what they are signing up for.
What to Expect at Your Evaluation
A proper dry eye work-up at our office is not a five-minute look-and-prescribe visit. It is a dedicated evaluation that typically includes:
- Symptom questionnaire (OSDI or SPEED) to score severity and baseline your symptoms
- Tear film analysis — osmolarity, tear break-up time, and staining patterns to classify evaporative vs. aqueous-deficient dry eye
- Meibography — digital imaging of your meibomian glands to quantify dropout
- Lid margin and Demodex exam — cylindrical collarettes, telangiectasia, and gland capping are all graded
- Personalized treatment plan — matched to your phenotype, skin type, and goals
If scleral lens therapy also makes sense as an adjunct for severe surface disease, we will walk you through that pathway too. For some patients with advanced MGD and significant corneal compromise, a combination of IPL, LipiFlow, and scleral lenses delivers the best long-term comfort.
Dr. Bonakdar's Approach
Dr. Alexander Bonakdar has been treating complex ocular surface disease in Orange County for more than 35 years. He is a California-licensed optometrist and ABO Board-Certified. Our office does not push a single device — we select the therapy (or combination) that matches your glands and your lifestyle.
Ready to find out which treatment your glands actually need? Call (949) 323-3600 to schedule your comprehensive dry eye evaluation at EyeCare Center of Orange County. We serve patients from Santa Ana, Irvine, Tustin, Newport Beach, and across Orange County.
Doctor-Recommended Dry Eye Products
Shop preservative-free artificial tears, lid hygiene products, and warm compress masks at our online store.
Shop DryEyeLA Products →¿Tiene preguntas sobre su salud visual?
El Dr. Alexander Bonakdar y su equipo están aquí para ayudarle. Agende una consulta para hablar sobre sus necesidades específicas.